Endometrial Cancer
Endometrial Cancer
The endometrium is the inner lining of the uterus, a hollow, muscular organ in a woman's pelvis. Endometrial cancer begins when cells in the endometrium starts to grow in an unregulated way. Cancer can grow in any part of the body, and can spread to other organ. This is also called as metastasis. In later stages, endometrial cancer can spread to the vagina, fallopian tubes, ovaries, bladder or rectum. It can also be spread to more distant organs. It is the second most common gynaecological malignancy with an incidence of 5.9 per 100,000 women in most developing countries.

Types
There are numerous different types of endometrial cancer based on how the cells look under the microscope.
They include:
Risk factor
Anything that increases your chance of getting a disease is called as risk factor. In more than 95% of cases, endometrial cancer happens in women over 40 years of age. Postmenopausal women are at high risk of getting endometrial cancer if they:
Symptoms

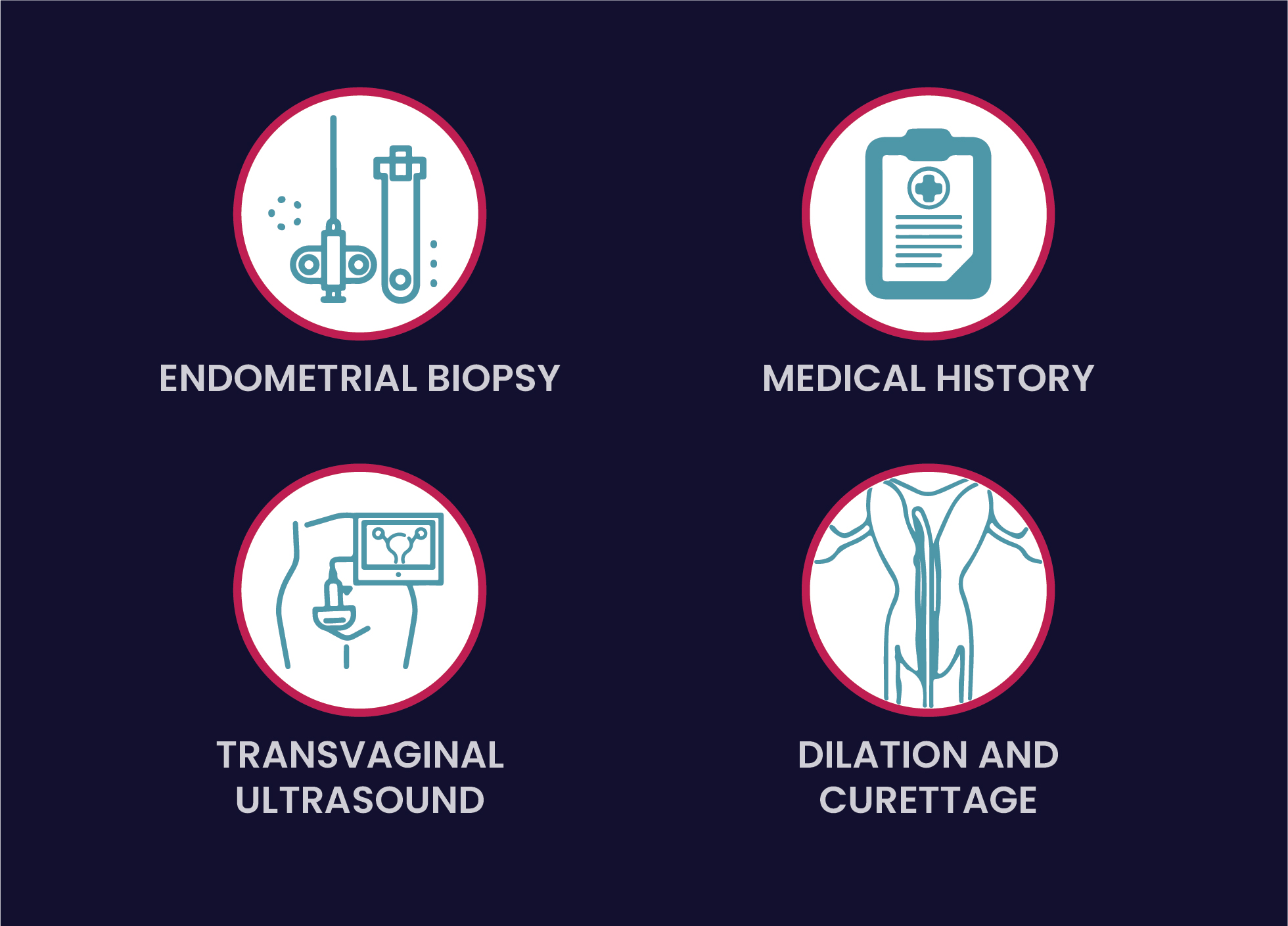
Diagnosis
If women have any of the above mentioned symptoms, their healthcare professional will examine them and possibly order blood and urine tests.
Other important tests include
Treatment
Surgery is often the main treatment for endometrial cancer that has not spread. It is also an effective prevention for women at high risk of developing the cancer. The most successful treatment for early cancer is total hysterectomy with bilateral salpingo-oophorectomy, in which the uterus, cervix, ovaries, and fallopian tubes are removed. This surgery is most likely to prevent the cancer from coming back.
If the cancer has spread outside the uterus, then after surgery the patient is given radiotherapy, often in combination with chemotherapy, to kill tumor is large but has not spread outside the uterus.
Patients with extensive endometrial cancer usually receive hormone therapy, usually progesterone, to delay the growth of cancer. Chemotherapy or radiotherapy might also be given to reduce the size and number of tumors - all of which can increase the survival rate and relieve symptoms.
Patients in remission need examination every few months for several years. If cancer comes back, it usually happens within three years. Caught early, cancer that comes back may be cured with aggressive radiation, chemotherapy, or more surgery.
To help cope with the emotional difficulties of having uterine cancer, patients might consider joining a support group. Counseling is helpful for pre-menopausal women who become depressed after a hysterectomy.